INTRODUCTION
Hiccup or hiccough is known by the medical term “singultus,” which is a derivative of the Latin word “singult,” meaning “a gasp” or “a sob” [1]. Hiccups are characterized by involuntary, intermittent, repetitive, myoclonic, and spasmodic contractions of the diaphragm and the inspiratory intercostal muscles, leading to an abrupt and early closure of the glottis, terminating inspiration and generating the characteristic “hic” sound [2,3]. Both healthy adults and children commonly experience hiccup spells. In the fetus, hiccups play a physiological role by training the respiratory muscles for their breathing function, and as a reflex preventing amniotic fluid aspiration [4,5]. Transient episodes usually do not require medical attention unlike chronic hiccups (persistent and intractable), which can be associated with long term deleterious effects.
An accurate estimate of the burden of hiccups in the neuro-intensive care unit (ICU) leading to unfavorable outcomes and morbidity is unknown. Though persistent hiccups which are intractable and of neurogenic origin can result in hyperventilation and respiratory alkalosis, and are a risk factor for ventilator associated pneumonia in intubated and mechanically ventilated patients. Hence, meticulous evaluation and treatment of persistent or intractable hiccups (IH) in neuro-ICU patients is important, in a stepwise and protocolized manner which comprise of physical maneuvers first followed by pharmacological measures in failed or resistant cases. Unfortunately, there are no clear guidelines applicable to the management of persistent or IH. Recently U.S. Food and Drug Administration (FDA) revoked the approval of chlorpromazine, citing its serious side effects in treating hiccups. In this article we strive to review the available literature on hiccups and provide a stepwise management protocol.
A single episode of hiccups can last from a few seconds to as long as several days. Based on the duration, hiccups can be divided into three categories: acute hiccups that last for up to 48 hours, persistent or protracted hiccups that last for more than 48 hours, and IH that last for over a month [6,7]. Most classifications use arbitrary time limits to categorize the phenomenon. Brief episodes of hiccupping are physiological. The point of transition to a pathological form is not well defined. The longer the duration of the hiccupping, the less amenable it will be to interventions. An episode lasting longer than a week is considered chronic while resistance to sequential therapy using three different drugs warrants the use of the label obstinate [8].
EPIDEMIOLOGY
Hiccups are more common in diseases affecting the gastrointestinal or central nervous system (CNS). Gender differences in hiccups frequency have not been seen in healthy subjects. Prevalence of non-CNS origin hiccups is higher in men than CNS origin hiccups [9,10]. No racial, geographic, or socioeconomic variation in hiccups has been documented. Recurrent hiccups occur in about 3% of the healthy population, compared to approximately 20% with Parkinson disease and 10% of patients with gastroesophageal reflux disease (GERD) [11]. Overall, the prevalence of hiccups in advanced cancer has been reported to be 3.9%–4.8% [12,13]. A variety of CNS pathologies cause IH. Lateral medullary infarcts (LMIs) cause 12%–36% of central hiccups cases. Keane (1961) found 56% of patients with central hiccups to primarily have LMIs, [14] and this proportion was 14% as per the report by Park et al. [15]. There is high preponderance of developing IH following an ischemic insult to the brainstem including pons or involvement of posterior inferior cerebellar artery [16,17]. Vascular lesions of CNS are the most common cause of IH followed by infective (meningitis, encephalitis), structural lesions, such as a multitude of space occupying lesions like cavernous angiomas or tuberculomas, and inflammatory and demyelinating conditions such as multiple sclerosis and neuromyelitis optica [18].
PATHOPHYSIOLOGY
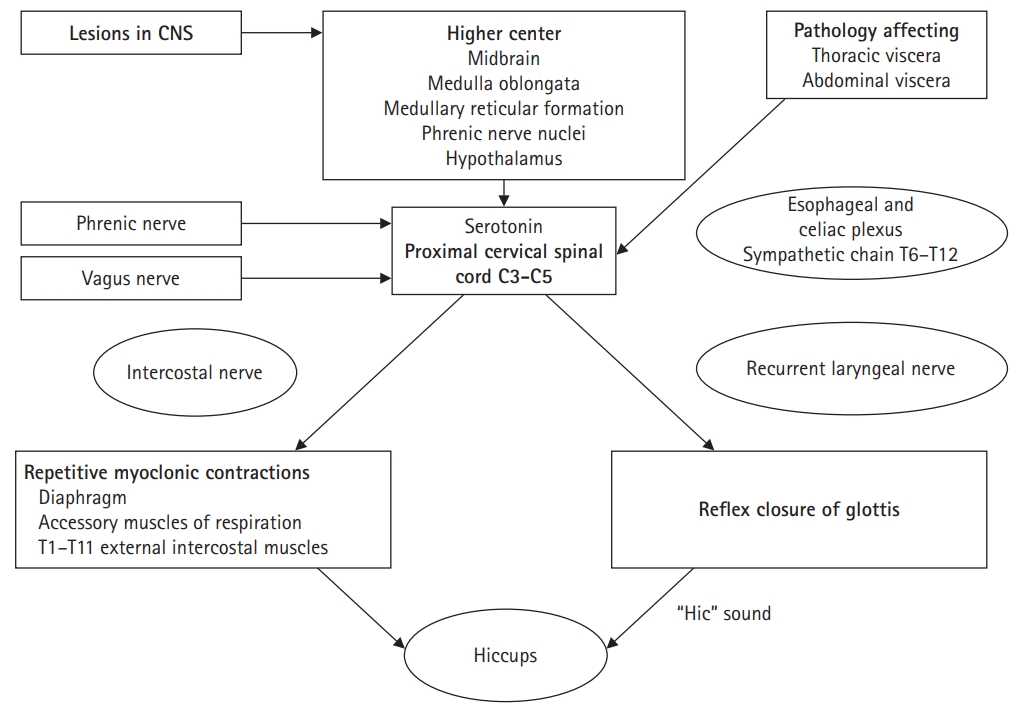
The mechanism of hiccups is not very clear and the neuroanatomical center for hiccups has not been identified, though few hiccups provoking hypothesis have been proposed [19,20]. Bailey [21] first proposed the “reflex arc” in 1943 responsible for generating hiccups. The afferent impulse in this proposed arc is carried by the vagus nerve, phrenic nerves, or sympathetic nerve fibers (thoracic outflow T6–T12). Upper spinal cord (C3–C5), medulla oblongata near the respiratory centers, the reticular formation, and the hypothalamus appear to be the CNS centers involved in the hiccup response. Dopaminergic and gamma-aminobutyric acid (GABA)ergic neurotransmitters are involved in the modulation of this central mechanism [22]. The efferent response of the reflex is carried by the phrenic nerve to the diaphragm. Accessory nerves activation lead to the contraction of the intercostal muscles as well. Recurrent laryngeal nerve causes the reflex closure of the glottis, completing the sequence of events during a hiccup [22,23]. Davis concluded that hiccup generation was a supraspinal mechanism involving interplay between behavioral and chemical respiratory influences at the spinal level, independent of inspiratory centers [24]. Suppression of inhibitory influences on a supraspinal hiccup center could lower the threshold and cause hiccups to start. This mechanism may explain the persistent hiccups seen in multiple sclerosis or metabolic disorders. Hassler [25] propounded that hiccups may be generated at the pontomedullary level of the triangle of Guillain-Mollaret (inferior olivary nucleus, dentate nucleus, and red nucleus). Denervation super sensitivity of the inferior olivary complex, nucleus ambiguus, and adjacent reticular formation of medullary oblongata have also been hypothesized to give rise to hiccups [26-28]. Nucleus raphe magnus with its GABA-containing inhibitory cells has been shown to be the likely source of inhibitory inputs to the hiccup reflex arc [29]. Various neurotransmitter pathways of the brainstem and medulla, including those involving dopamine, serotonin, opioids, calcium channels, and GABA are possibly involved in mediating hiccups [30] (Fig. 1).
ETIOLOGY
Any process that affects the peripheral afferent, central, or efferent components of the proposed reflex arc can trigger hiccups [22]. The most common benign reason being large meals or carbonated drinks causing stomach distension. Hot and spicy foods, alcohol, smoking, and other substances irritating the gastrointestinal or pulmonary tracts can also trigger the reflex. Over-excitement or anxiety, when accompanied by hyperventilation or air swallowing (aerophagia) can trigger hiccups as well.
The causes of persistent hiccups can be classified into central and peripheral (Table 1). Central hiccups could occur with any lesions along the pathway from the CNS to the phrenic nerve, especially with lesions of the brain stem, such as tumors and ischemic stroke [15,17,18,31]. Peripheral hiccups can be caused by diseases at the phrenic nerve level involving diaphragmatic irritation, such as gastric distention, subdiaphragmatic abscess, or hepatosplenomegaly.
Cns Lesions
The dorsal area of the medulla is commonly associated with hiccups as it incorporates a number of complex structures which conciliate the reflex arc, including the vagus nerve, respiratory center, solitary nucleus, nucleus ambiguus, central sympathetic tract, and spinal tract of trigeminal nucleus. Chronic hiccups have been reported following hemorrhagic and ischemic strokes, cerebellar aneurysms, and neuromyelitis optica [32-38].
Peripheral nervous system lesions
Involvement of the hiccup reflex arc in conditions like sarcoidosis, diaphragm tumors, or other causes of abdominal distension may lead to persistent hiccups.
Hiccups under anesthesia
Hiccups can occur during administration of general or regional anesthesia [42], particularly under lighter plane of anesthesia especially with the usage of short acting barbiturates and during intubation, patient positioning, or visceral manipulation during surgery. Surgeries in thorax and abdomen often lead to hiccups in the postoperative period probably due to gastroparesis [43]. Anesthetic drugs like propofol induced hiccups [44]. Hiccups following epidural anesthesia have been reported with possible mechanism of action being deafferentation of sensory nerves in the viscera coupled with increased diaphragmatic stimulation secondary to interruption of phrenic nerve motor reflex [45,46].
Cancer patients
Hiccups are frequently seen in patients with cancer either due to involvement of any portion of the hiccup reflex arc by the tumor, or as a secondary response to chemotherapy. Cisplatin is most commonly implicated [47].
Drug-induced hiccups
Steroids have been implicated in chronic hiccups. Dopamine agonists may induce bouts of hiccups in Parkinsonism patients owing to their high affinity towards D3 receptors. Macrolides like azithromycin and psychiatric medications like aripiprazole have also been known to be associated with persistent hiccups. In essence, it is imperative to thoroughly review the medication history and identify and stop the offending drugs inducing hiccups [48].
Instrumentation-associated hiccups
Atrial pacing, catheter ablation of atrial fibrillation, and central venous catheter placement have been reported to cause hiccups presumably due to mechanical irritation of right phrenic nerve which is in close proximity to the right atrium [49-51]. Esophageal instrumentations like stenting induces hiccup by stimulating the reflex arc afferent component [52].
Psychogenic causes
Hiccups are seen in patients with acute anxiety, stress, fear, or excitement. In cases where behavioral therapy has been successful in ameliorating hiccups, a diagnosis of hysterical hiccups has been made [53].
Miscellaneous causes
Dyselectrolytemias, tuberculosis, ethanol abusers, diabetes mellitus, and chronic renal failure (due to uremia) [54] can all cause persistent hiccups. Electroencephalogram findings in patients with epilepsy suggest that chronic hiccup can be the result of seizure activity. Certain antiepileptic drugs have shown a beneficial role in the treatment of hiccups mainly due to their GABAergic effects. However, in many patients, chronic hiccups occur without the presence of cerebral dysfunction and diazepam, a potent anti-convulsant drug, can precipitate or exacerbate hiccups in such conditions [55].
EFFECTS OF PERSISTENT HICCUPS
Persistent hiccups have the capacity to induce major disabling impact on general health and cause exhaustion, sleep deprivation, malnutrition, dehydration, depression, wound dehiscence, and even death in extreme cases [2,56]. It has a detrimental effect on rehabilitation as shown by prolonged hospital stay in a study done by Kumar and Dromerick [16]. Sleep cycle is affected by hiccups with literature showing that it persists during sleep disrupting both non-rapid eye movement (NREM) and REM sleep. Chronic hiccups lead to sleep deprivation [57].
EFFECTS OF HICCUPS ON RESPIRATION
The occurrence of hiccups in a patient receiving mechanical ventilation causes desynchronization and possible respiratory alkalosis leading to lung damage and hemodynamic alterations [58]. It can be prevented by close monitoring of respiratory parameters and prompt correction, especially in patients with brain stem damage. The strong inspiratory effort does not result in a large change in lung volume due to reflex glottic closure, and, therefore, in normal subjects the ventilatory effects of hiccups are minimal. In intubated or tracheostomized patients, hyperventilation and respiratory alkalosis may happen resulting in hiccups [59].
Marinella [2] were able to demonstrate that the left hemi-diaphragm was the side of hiccup origin in 80% of their cohort of patients with advanced malignancy. Persistent and IH are a risk factor for ventilator-associated pneumonia in intubated patients. Employing continuous positive airway pressure and pressure support ventilation can stop hiccups in such patients. Salem et al. [60] demonstrated that increasing PIP to 30–40 cmH2O immediately stopped the development of hiccup during a surgical procedure.
EVALUATION
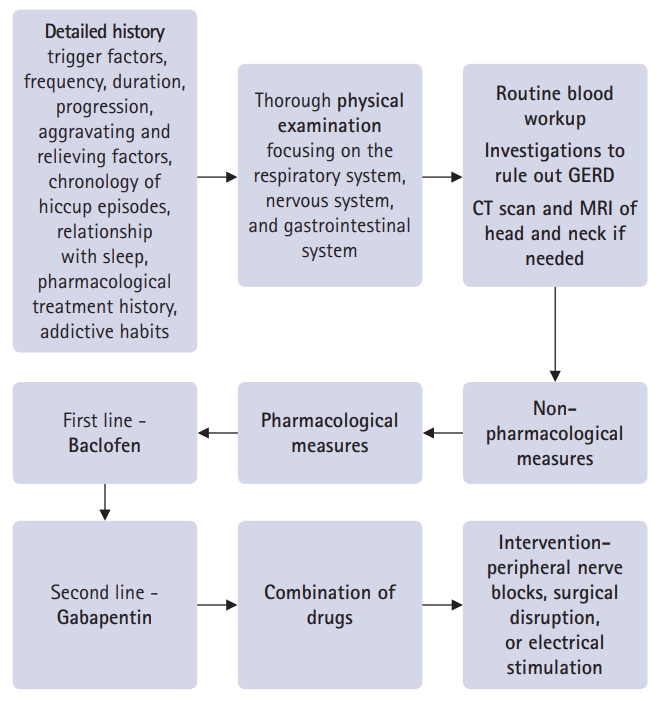
A thorough and detailed history is warranted focusing on trigger factors for chronic hiccups along with frequency, duration, progression, and aggravating and relieving factors. Relevant history should be elicited regarding the chronology of hiccup episodes, relationship with sleep, and any physical maneuver or pharmacological treatment the patient is undergoing with their effectiveness on the condition and any side effects experienced. A comprehensive enquiry should be made regarding the prescribed medications the patient has been administered along with over-the-counter medications and various addictive habits, such as smoking and alcohol consumption. An underlying organic pathology should be ruled out in patients with chronic hiccups.
A detailed physical examination should be done along with a systemic one focusing on the respiratory, nervous, and gastrointestinal systems. An electrocardiogram may help rule out atypical myocardial infarction especially in the beginning of a hiccup attack. Routine blood workup should be done including complete blood count, electrolytes, blood urea nitrogen, creatinine, calcium, liver function tests, and amylase/lipase. Investigation to rule out GERD is important and includes an upper gastrointestinal endoscopy, esophageal manometry, and a 24 hour–pH-impedance reflux study [61]. In patients where no organic cause can be found or those not responding to routine treatment, imaging studies like computed tomography scan and magnetic resonance imaging of head and neck are warranted [62]. Stepwise management protocol is given in flow diagram (Fig. 2).
TREATMENT
The treatment approach of persistent hiccups is mostly based on observational reports and case series, and clear-cut guidelines are lacking. The treatment is mainly directed at treating the underlying cause when the illness causing hiccups has been identified [2,22,23]. In majority of the cases, no cause is found and the treatment is mainly empirical to ameliorate the symptoms. Table 2 shows the anecdotal and nonpharmacological treatment methods. Physical maneuvers such as interrupting normal respiratory function (e.g., breath holding, Valsalva maneuver), stimulating nasopharynx or uvula (e.g., sipping cold water, gargling with water, swallowing a teaspoon of dry sugar), increasing vagal stimulation (e.g., pressing on the eyeballs), and countering irritation of the diaphragm (e.g., pulling knees to chest, leaning forward to compress the chest) are first-line treatments for hiccups. The basic principle of the various physical maneuvers employed is to interrupt or suppress the reflex arc [7]. These, at best, provide a transient relief in cases of persistent or IH. Drug therapy should be reserved for treatment of hiccups when physical maneuvers have failed [63,64].
Pharmacological
There is inadequate data to formulate treatment guidelines for persistent hiccups [57]. A complete medical history regarding the ongoing medications and comorbid conditions should be available, and the possible drug interactions and probable side effects should be kept in mind before the choice of medication is made. Combination therapy for IH has also been proposed in certain case reports [65]. The drug therapy could be tapered out or discontinued if hiccups cease, and alternative drug or treatment modality could be considered in case of IH. The pharmacological treatment is summarized in Table 3.
Chlorpromazine
Chlorpromazine, a dimethylamine derivative of phenothiazine, is a centrally acting dopamine antagonist which acts at the hypothalamus. The concerns pertaining to long-term neurological side effects along with hypotension, urinary retention, glaucoma, or delirium associated with the use of chlorpromazine has led to its U.S. FDA approval recently being withdrawn. The suggested dose has been 10–25 mg orally or intravenously; if no response then up to 25–50 mg three times a day can be used [66]. Other neuroleptics, like haloperidol or olanzapine, though effective are limited by their untoward effects such as such as dizziness, mood disturbance, and sedation.
Haloperidol
It alleviates hiccups by its dopamine antagonism in the hypothalamus. The major side effect is extrapyramidal symptoms. Recommended dosage is 5–10 mg/day orally or 2 mg intramuscularly [67].
Olanzapine
Postsynaptic serotonergic receptors augment phrenic motoneuronal activity and play a role in the generation of hiccups. Olanzapine is proposed to act as an antagonist at these postsynaptic receptors, thereby, attenuates phrenic excitability and relieves hiccups. Alderfer and Arciniegas [68] reported that a maintenance dose of 2.5 mg once daily led to remission of IH secondary to brain injury.
Benzodiazepines
High-dose benzodiazepines can alleviate treatment-resistant hiccups by suppressing the repetitive, myoclonic contractions of the diaphragm. Midazolam is used via continuous infusion at the rate of 10–60 mg/24 hr in patients with terminal hiccups, in the context of refractory delirium or agitation [69].
Muscle relaxants
Baclofen
Baclofen, a GABA-B agonist, inhibits transient relaxations of the lower esophageal sphincter and diaphragm with its peripherally and centrally mediated effect on vagal nerves. It also affects the esophago-gastric junction and suppresses reflux after meals. Concerns with its use include ataxia, confusion, and sedation especially in elderly patients with renal failure. Dose is 5 mg per 12 or 8 hours to start with, progressively increased by 15 mg every 3 days to a maximum daily dosage of 75 mg till optimal dose is reached [70-72]. Treatment should be slowly tapered over several days and never abruptly stopped.
Anti-epileptic drugs
Anti-convulsant medications are used as a second line treatment of persistent hiccups. They block the excitatory neural sodium channels (e.g., phenytoin, carbamazepine), enhance the release of GABA, and decrease the release of excitatory neurotransmitters in the CNS.
Gabapentin
Gabapentin modulates diaphragmatic excitability by increasing the endogenous GABA-mediated inhibition of inspiratory muscles and reducing calcium influx through inhibitory effects on voltage-operated calcium channels in the presynaptic terminals of respiratory muscles. It also increases serotonin levels in the nucleus raphe magnus of the medulla, which is the most likely source of GABAergic inhibitory inputs to the hiccup reflex arc. Gabapentin either alone or in combination with other medications has been recommended especially in patients with hiccups secondary to brain tumors. Gabapentin dosage is 300 mg three times daily orally and titrated according to response, or 400 mg three times daily for 3 days, then 400 mg once daily for 3 days, and then stopped [73]. Porzio et al. [12] in their retrospective study evaluated gabapentin’s efficacy in patients with advanced cancer having severe chronic hiccups and concluded that gabapentin can be used as a next line therapy to chlorpromazine. It has a favorable side effect profile compared to other anti-epileptic drugs.
Valproic acid
Valproic acid increases the GABA transmission centrally and interrupts the hiccup stimuli. It is associated with serious side effects like gastrointestinal bleeding and hepatic toxicity. Recommended dosage is 200–500 mg orally (15 mg/kg/24 hr in divided doses) [75].
Metoclopramide
It is a D3 antagonist and 5-HT4 agonist with a chemical structure similar to neuroleptic drugs. It has both central anti-emetic and peripheral prokinetic properties with a lower esophageal sphincter tightening effect. Its efficacy in hiccups is due to gastric emptying because of its prokinetic property, which reduces gastric distension and GERD. Recommended dose is 10 mg intravenously three to four times a day [76,77]. Wang and Wang [77] in their randomized study demonstrated its benefit on terminating hiccups. Long-term dosing is associated with risk of tardive dyskinesia.
Domperidone
The drug is devoid of neurological side effects associated with metoclopramide as it does not cross the blood-brain barrier. It has a better risk profile over a longer period of time but there are concerns with its propensity to cause QT interval prolongation and cardiac dysrhythmias. The dosage is 10 mg three to four times a day [65].
Cisapride
It has 5-HT4 agonism and an effect comparable to metoclopramide. Dosage is 10 mg three times a day, taken orally [78].
Nifedipine
It is a calcium channel blocker and interrupts the reflex arc by reversing the abnormal depolarization, with the major side effect being hypotension. Recommended dosage is 10 mg orally three times a day with concurrent fludrocortisone 0.5–1 mg orally [79].
Methylphenidate
It terminates hiccups through inhibition of dopamine and norepinephrine reuptake. In the case report published by Maréchal et al. [80], methylphenidate was effective in terminating hiccups in a patient with metastatic small cell lung cancer with a dose of 5 mg orally (maintenance 5–10 mg twice daily).
Nefopam
It is a non-opioid analgesic with reported efficacy in terminating refractory hiccups with intravenous medication at a dose of 0.25 mg/kg over 10 seconds (10 mg intravenously four times daily for 2 days) [81].
Carvedilol
Carvedilol suppresses hiccups by acting on the afferent sympathetic component of the reflex arc. Stueber and Swartz [82] reported that it was effective in treating hiccups in a patient with tardive dyskinesia and compulsive self-induced hiccups and vomiting, at doses of 6.25 mg four times daily.
Lidocaine
Lidocaine nebulization is found to be effective in treating hiccups due to its effect on irritant sensory afferents. The safety profile with this is considerably better as compared to intravenous route which is fraught with neurological and cardiovascular toxicities [83,84]. Kaneishi and Kawabata [85] reported a case of hiccups, resistant to haloperidol, effectively treated by lignocaine.
Amantadine
Amantadine is an antagonist at the NMDA receptors with anticholinergic activity and anti-Parkinsonian effect and possible anti-hiccup action. There are case reports regarding the onset of hiccups following administration of dopamine agonists in a patient with Parkinson disease [86].
Combination therapy for IH
Combination therapy for IH has also been proposed in certain case reports [65].
Cisapride, omeprazole, and baclofen (COB)
Petroianu et al. [87] studied oral treatment with cisapride 10 mg three times daily, omeprazole 20 mg once daily, and baclofen 15 mg three times daily in patients with IH and concluded that COB is an effective empirical therapy.
Cisapride, omeprazole, baclofen, and gabapentin
In another study, Petroianu et al. [88] proposed that the addition of gabapentin should be considered in patients for better results.
CONCLUSION
Hiccups are usually innocuous and frequently ignored. Patients presenting with chronic hiccups require a meticulous evaluation focusing on history and physical examination. Persistent hiccups are more often than not associated with an underlying organic pathology which requires a comprehensive workup. Pharmacological therapy should take into account the risk of long-term side effects and FDA recommendations. Considering the present literature on hiccup pharmacotherapy, baclofen may be considered as a first line therapy followed by gabapentin. Large multicenter trials are the need of the hour along with the development of robust guidelines.