Is the mechanism of synchronous cardiocerebral infarction (CCI) different from that of metachronous CCI?
Article information

Abstract
Background
Cardiocerebral infarction (CCI) is the simultaneous occurrence of acute ischemic stroke (AIS) and myocardial infarction (MI) at the same time (synchronous), or one after another (metachronous). This study aimed to investigate the differences in the underlying mechanisms between synchronous and metachronous CCI.
Methods
This study analyzed patients with AIS registered in the Clinical Research Collaboration for Stroke in Korea Prospective Registry at a single Stroke Center from January 2019 to December 2022. Patients with synchronous and metachronous CCI (MI within 72 hours after AIS) were included. Severity at admission and modified Rankin Scale scores 3 months after treatment were assessed.
Results
Among 3,319 AIS patients, 12 (0.36%) were diagnosed with acute CCI (male, 8; mean age, 69.6±14.0 years). Of these, six (0.18%) had synchronous CCI, while the other six had metachronous CCI. The synchronous CCI group exhibited lower neurological severity at admission than the metachronous CCI group (median National Institutes of Health Stroke Scale, 3.5 vs. 12.5). Among the 12 patients, seven (58%) had ST-elevation myocardial infarction (STEMI), with five (83%) of the synchronous CCI cases presenting as STEMI. Two cases of new-onset atrial fibrillation occurred exclusively in patients with synchronous CCI. Also, one case with synchronous CCI had a thrombus in the left ventricle.
Conclusion
Acute CCI is rare and manifests with varying degrees of severity. Our study suggests that AIS in synchronous CCI may be secondary to embolism caused by a preceding MI. In contrast, metachronous CCI exhibits diverse mechanisms, including secondary myocardial injury resulting from a preceding severe AIS.
INTRODUCTION
Acute cardiocerebral infarction (CCI) is a rare, life-threatening condition in which both acute ischemic stroke (AIS) and myocardial infarction (MI) occur simultaneously [1,2]. Recently, researchers categorized acute CCI into two subtypes based on the timing of its occurrence: synchronous CCI and metachronous CCI [3]. Synchronous CCI is a simultaneous infarction in the cerebral and coronary vascular territories, whereas metachronous CCI occurs when one event precedes the other, regardless of the order of AIS and MI [2]. Metachronous CCI has been documented to occur in a range of 0.9% to 12.7% [4,5], whereas synchronous CCI is extremely rare, with a prevalence rate of 0.9% [6]. In particular, in a 3-year prospective study of patients with acute cerebrovascular accidents admitted to a geriatric unit within 72 hours of onset, 12.7% were found to have what was considered to be associated with acute MI [7].
Prompt intervention and revascularization are essential for optimal treatment of both AIS and MI. However, there are currently no definitive guidelines for determining the priority of treating one condition over another. Although there are similarities in the treatment approaches for AIS and MI, slight variations in reperfusion treatment indications, medications, and dosage selection can add complexity to the emergency physician’s decision-making process and hinder prompt decision making [3].
For these reasons, the mortality rate associated with acute CCI is high. However, comprehensive studies regarding this condition are lacking [8]. Furthermore, despite the distinct differences in the timing of occurrence between synchronous and metachronous CCI, it remains unclear whether there is a difference in the underlying mechanisms between these two forms of CCI. To address these uncertainties, we aimed to determine the underlying mechanisms of the two distinct forms of acute CCI, synchronous CCI and metachronous CCI, by analyzing the clinical characteristics, patterns of MI occurrence, mechanisms of AIS, and outcomes of acute CCI patients enrolled in the Clinical Research Collaboration for Stroke in Korea (CRCS-K) registry [9] at a single Stroke Center.
METHODS
This study focused on patients with AIS who were prospectively registered in the CRCS-K registry at a single Stroke Center between January 1, 2019, and December 31, 2022. This study complied with the principles of the Declaration of Helsinki.
We included adults aged 18 and above, who were diagnosed with AIS and MI. The times of occurrence and hospital admission for AIS and MI were recorded. The timing of AIS occurrence was determined based on the onset time of neurological symptoms or the last normal time, whereas the timing of MI occurrence was established using clinical symptoms, cardiac enzyme elevation, or evidence of MI on electrocardiography or echocardiography.
The participants were categorized into two groups based on the timing of occurrence. Patients who exhibited both AIS and MI simultaneously upon arrival at the emergency room were grouped as having synchronous CCI. In contrast, patients who developed MI within 72 hours of admission for AIS were grouped as having metachronous CCI. The interval between AIS and MI in metachronous CCI was determined as described by Chin et al. [7].
Demographic data, vascular risk factors, medical history, including atrial fibrillation, coronary heart disease, and prior antithrombotic use were investigated. The severity of stroke upon admission in patients with AIS was assessed using the National Institutes of Health Stroke Scale (NIHSS). Stroke type was classified according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification with certain modifications. The TOAST classification was applied using a magnetic resonance imaging-based algorithm for AIS subtype classification (MAGIC) [10]. All patients with CCI experienced recent MI, which could be regarded as a major source of cardioembolism. However, only cases that met the differential criteria outlined by MAGIC were considered to have cardioembolic mechanisms.
We collected laboratory test results, including cardiac troponin I levels, which were within the normal range (<0.034 ng/mL). The type of MI (ST elevation and non-ST-segment elevation) was noted. Ejection fraction (EF) was classified into preserved (EF ≥50%), mid-range (40%–49% EF), and reduced (<40% EF), and presence of thrombus was confirmed on echocardiogram in the emergency room.
We reviewed the implementation of reperfusion therapies such as intravenous thrombolysis, mechanical thrombectomy, and percutaneous coronary intervention. We also investigated whether craniectomy could be performed due to the progression of brain edema in patients with malignant cerebral infarction. The functional and mortality outcomes of the participants were analyzed using the modified Rankin Scale (mRS) score at the 3-month follow-up after hospital admission. A poor functional outcome was defined as an mRS of 3–6. The cause of death was determined and documented in the deceased patients.
Variables were summarized as frequency and percentage for categorical data and mean±standard deviation and median (range) for numeric data. Group differences were tested using Fisher’s exact test for categorical data and the Mann-Whitney U-test for numeric data, as appropriate. Outcome incidence rates according to the CCI group were analyzed using Exact Poisson Regression. All statistical analyses were performed using STATA 18.0, statistical software (StataCorp.), and a P-value less than 0.05 was considered statistically significant.
RESULTS
During the study period, 3,319 patients with AIS were registered in the CRCS-K registry at a single Stroke Center. Among these, 12 (0.36%) were diagnosed with acute CCI. Of these, six patients (0.18%) were classified into the simultaneous CCI group, and the remaining six patients (0.18%) were classified into the metachronous CCI group (Table 1). Among the 12 patients with acute CCI, 7 had ST-elevation myocardial infarction (STEMI), while the remaining 5 had non–ST-elevation myocardial infarction (NSTEMI). The mean age of the 12 patients with acute CCI was 69.6±14.0 years, and the initial median NIHSS was 5, ranging from 0 to 18. The average time from onset-to-door for these patients was 531.7±511.8 minutes, ranging from 57 to 1,440 minutes.
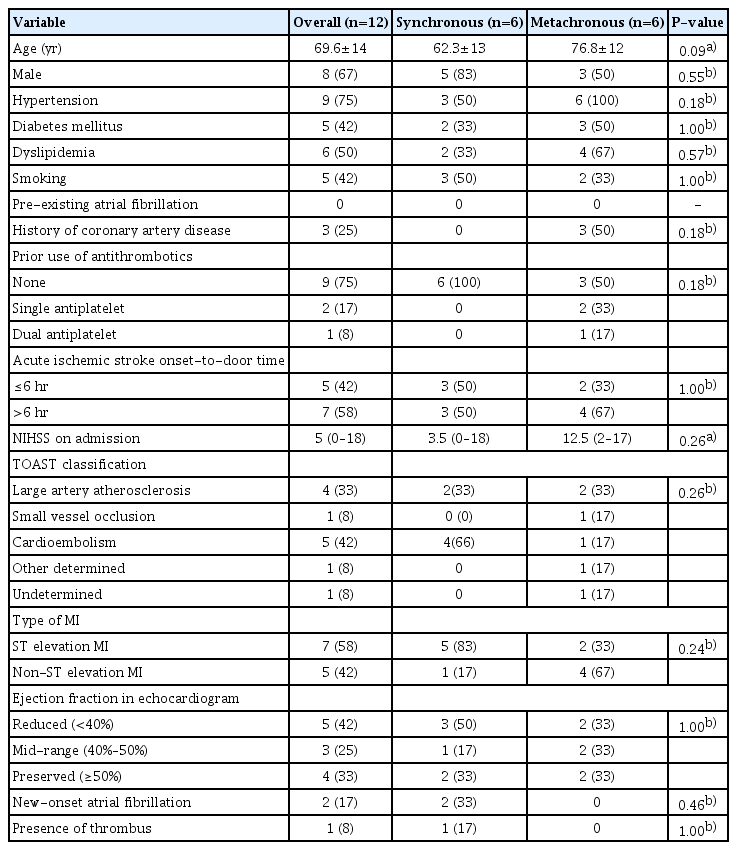
Clinical profile of patients with cardiocerebral infarction
When comparing basic demographics, clinical characteristics, and laboratory findings between patients with synchronous and metachronous CCI, no statistically significant differences were observed. However, patients with metachronous CCI had a higher prevalence of advanced age, greater burden of vascular risk factors, and a higher incidence of previous antithrombotic medication use than those with synchronous CCI. Additionally, synchronous CCI patients, with an initial median NIHSS score of 3.5, tended to have lower neurological severity at admission than metachronous CCI patients, whose initial median NIHSS score was 12.5. According to the MAGIC classification, synchronous CCI is more often associated with cardioembolism than with other mechanisms. Furthermore, the synchronous CCI group exhibited a higher incidence of STEMI than the metachronous CCI group. In our study, both cases of new-onset atrial fibrillation occurred in patients with synchronous CCI. Additionally, a left ventricular thrombus was observed in one patient with synchronous CCI on echocardiography. We also detailed the clinical characteristics of the 12 patients diagnosed with CCI (Table 2).

Clinical features data for 12 patients with CCI
Reperfusion therapy for AIS was administered to six individuals (50%), four of whom had metachronous CCI (Table 3). Craniectomy was performed in one patient with metachronous CCI. All patients with acute CCI underwent percutaneous coronary intervention. No statistically significant differences were observed when comparing reperfusion therapy between synchronous and metachronous CCI.

Management of cardiocerebral infarction
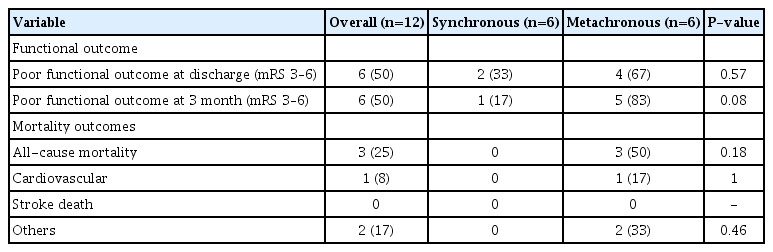
In the assessment of the functional outcome of 12 cases of acute CCI at 3 months, six patients (50%) experienced a poor outcome, as indicated by an mRS score of 3 to 6 (Table 4). Notably, the rate of poor functional outcomes at three months was higher in the metachronous CCI group (83%) than in the synchronous CCI group (17%). Mortality occurred in three cases, all of which were observed in patients with metachronous CCI. One of these three patients died from cardiovascular causes, while the other two patients died from sepsis. There were no statistically significant differences according to Fisher’s exact test. We conducted exact Poisson regression analysis to further evaluate the outcomes. The incidence of poor functional outcome at discharge was higher in metachronous CCI group compared with synchronous CCI group (relative risk [RR], 2.00; 95% confidence interval [CI], 0.29–22.11; P=0.69) Also, the incidence of poor functional outcome at 3 months was higher in metachronous CCI group compared with synchronous CCI group. (RR, 5.00; 95% CI, 0.56–236.49; P=0.22) Finally, the incidence of all-cause mortality was higher in metachronous CCI group compared with synchronous CCI group. (RR, 3.85; 95% CI, 0.41–infinite; P=0.25) Although there were no statistically significant results, it was confirmed that the metachronous CCI group had a higher incidence of poor functional outcomes.
Outcomes of patients with cardiocerebral infarction
DISCUSSION
Our study showed that the incidence of acute CCI was 0.36%, with synchronous CCI accounting for 0.18% of the cases, indicating a relatively rare occurrence. While the previously reported frequency of synchronous CCI is cited as 0.009% based on Yeo's publication, upon reviewing Yeo's report [6], it is evident that out of 555 patients with AIS, five cases of synchronous CCI were observed, resulting in an accurate figure of 0.9%.
In this study, several distinct differences were observed between synchronous and metachronous CCI beyond the timing of occurrence. First, patients with synchronous CCI were younger than those with metachronous CCI and exhibited lower neurological severity at the time of AIS occurrence. Second, the incidence rate of STEMI was higher in the synchronous CCI group (83%) than in the metachronous CCI group (33%). Third, new-onset atrial fibrillation and intraventricular thrombosis on echocardiography were only found in patients with synchronous CCI.
According to a previous report by Wang et al. [1], the pathogenesis of acute CCI can be categorized into two main mechanisms. First, it can be attributed to cardiac causes such as atrial fibrillation. Secondly, this may have resulted from brain causes. Specifically, in cases of brain damage, neurological damage caused by AIS is involved, and there is an interplay known as stroke-heart crosstalk, which includes the hypothalamic-pituitary-adrenal axis, immune and inflammatory responses, and various risk factors (such as age, sex, race, hypertension, smoking, diet, and physical inactivity) primarily involved in the pathogenesis of AIS [11,12]. Ultimately, these reactions act as cardiac burdens, leading to cardiac arrhythmias and potentially triggering MI. Indeed, myocardial damage following AIS is associated with specific brain regions such as the insular cortex. However, it is mostly observed in patients with moderate-to-severe AIS and typically occurs approximately 24 hours after stroke onset [13,14]. This suggests that metachronous CCI is associated with a higher risk of MI following a preceding stroke.
In this study, it was observed that the cardiac troponin-I levels were elevated in all acute CCI patients tested in the emergency room. Specifically, even in patients with metachronous CCI, these levels were elevated. Therefore, in patients with AIS presenting to the emergency room with an increase in cardiac troponin I levels, it is important to consider intensive cardiac evaluations, even in the absence of other findings suggestive of MI.
In this study, all three cases of new-onset atrial fibrillation occurred in patients with synchronous CCI. Atrial fibrillation has been reported as a potential cause of simultaneous CCI because it is a common source of both cerebral and coronary embolisms [4,6]. Furthermore, in synchronous CCI, echocardiography performed in the emergency room revealed the presence of a left ventricular thrombus in one patient. Additionally, the frequency of STEMI was significantly higher in the synchronous CCI group than in the metachronous CCI group.
When blood clots form at the site of cardiac muscle damage, they may cause left ventricular stenosis or a left ventricular thrombus. The incidence of left ventricular thrombus following acute MI is reported to be 20%–40%. In particular, patients with STEMI have been reported to be more likely to have a left ventricular thrombus than patients with NSTEMI (43.1% vs. 5.0%) [15]. Also, a left ventricular thrombus may be a potential risk factor for an embolic source. These findings suggest the possibility that synchronous CCI is caused by cardiac factors. However, more detailed research is required to clearly demonstrate this sequential relationship.
In this study, the mean age of patients with synchronous CCI was lower than that of patients with metachronous CCI. Considering the general fact that the average age of the patients with MI was lower than that of the patients with AIS, this suggests the possibility of a closer association between synchronous CCI and cardiac causes. Interestingly, despite the higher likelihood of synchronous CCI patients having conditions caused by cardiac factors, their neurological severity is comparatively lower, and most patients primarily complain of stroke symptoms, such as hemiparesis, rather than symptoms suggestive of MI. Symptoms such as chest pain, commonly associated with MI, may go unnoticed in stroke patients and can be attributed to the following factors. (1) Stroke-related brain damage can affect the central nervous system, leading to impaired transmission of sensory signals related to cardiac pain. (2) Stroke-induced changes in consciousness or a state of confusion can prevent the perception of cardiac pain [3,16].
In this study, 41.7% of patients with acute CCI received reperfusion therapy, such as intravenous thrombolysis or mechanical thrombectomy. This percentage was higher than that of the approximately 16% of patients who received reperfusion therapy based on the 2020 CRCS-K registry data [17]. This difference can be attributed to the fact that in this study, the average onset-to-door time for acute CCI patients was approximately 8 hours, which is significantly shorter than the average of 42 hours for all registered AIS patients in the CRCS-K registry. In a meta-analysis of Acute CCI [18], similar results were found, with over 50% of the patients with acute CCI receiving reperfusion therapy, as observed in our study.
Similar to previous studies, the frequency of poor outcomes at 90 days in patients with acute CCI in this study was >50% [3,6,18], which is higher than the 38.2% reported in the CRCS-K registry. The mortality rate was 25%, which is significantly higher than the 2.8% reported in the CRCS-K registry [17]. The high mortality rate in acute CCI can be attributed not only to the initial high severity upon admission and the higher frequency of reperfusion therapy but also to the delayed diagnosis of concomitant MI and a potential lack of comprehensive treatment guidelines for acute CCI. This delay in appropriate management could contribute to the higher mortality rates observed in patients with acute CCI.
In the present study, metachronous CCI was associated with poor functional outcomes and higher mortality rates. These results may be related to the neurological burden of the high NIHSS score and large size of the cerebral infarction in the metachronous CCI group. When the level of consciousness decreases, the airway is not protected, which increases the risk of aspiration pneumonia. In addition, severe neurological symptoms can aggravate underlying cardiac problems, resulting in death.
Our study has several limitations. First, we only included patients enrolled in the CRCS-K registry and there were no data on patients who developed AIS after MI. Second, the actual onset times of AIS and MI may differ even among the synchronous CCI groups because we classified CCI based on tests performed in the emergency room. Therefore, even if AIS and MI occur >12 hours apart, they can be classified as synchronous CCI.
This study reports a relatively rare case series of acute CCI prospectively tracked in a single-institution registry. In contrast to previous reports, MI can occur in AIS cases of varying severity and underlying mechanisms. Despite these findings, the prognosis of patients with acute CCI remains poor, with a high mortality rate. Therefore, there is a need to gather fundamental data through multicenter studies to develop response manuals and guidelines for acute CCI.
Notes
Ethics statement
The study protocol was reviewed and approved by the Institutional Review Board of Dong-A University on July 26, 2023 (No. 23-135). Written informed consent was obtained from all the participants.
Conflict of interest
Jin-Heon Jeong is an editorial board member of the journal but he was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflict of interest relevant to this article was reported.
Author contributions
Conceptualization: JKC. Methodology: SK, JHJ. Formal analysis: SK, HC. Data curation: DHK, BAY, YL. Visualization: SK, YL. Project administration: JKC. Writing–original draft: SK, JKC. Writing–review & editing: SK, JKC.